Imagine a future where genetic anomalies can be precisely targeted and corrected using genome editing – a giant leap from our ability to sequence or read human genomes two decades ago. The world of medicine is currently abuzz with news of regulatory agencies’ approval for two highly anticipated CRISPR-based therapies for sickle-cell disease and β-thalassaemia in the U.K. and the U.S.
The approval is groundbreaking because it augurs an era that could transform the lives of millions of patients and families grappling with these inherited blood disorders. To put this in perspective, more than a million people worldwide suffer from thalassemia, of whom 100,000 depend on regular blood transfusions. Another 20 million people around the world are estimated to be suffering from sickle-cell anaemia.
Long and short of CRISPR
The discovery of the CRISPR system was the result of almost three decades of pure academic pursuit. Clustered regularly interspaced short palindromic repeats (CRISPR) are DNA elements that Spanish researchers discovered in archaea in 1993, and named and described later in a number of bacterial genomes.
These elements contain pieces of genetic material derived from viruses that infect bacteria (i.e. bacteriophages) and a set of proteins called Cas, or CRISPR-associated. Researchers tried to explain the elements’ effect on antiviral immunity in 2005, but later found that CRISPR + Cas proteins could detect and prevent viral infections. That is, the two formed an antiviral defence system and helped bacteria ‘acquire’ resistance.
Then, in 2010, scientists demonstrated that CRISPR + specific proteins called Cas9 had the ability to cut double-stranded DNA at specific points. They also found the RNAs molecules that guided the Cas9 proteins to specific positions on a genome. And in 2012, researchers figured out a way to create synthetic RNA that could bind to Cas9 and guide it to a specific point on a DNA, where it could edit the DNA.
This pathbreaking work came from the labs of Emmanuelle Charpentier and Jennifer Doudna, and they were awarded the 2020 Nobel Prize in chemistry for it.
Virginijus Siksnys and his colleagues published similar work a few months later (despite having submitted it to the journal much earlier). This study also suggested that Cas9 could be targeted to specific genome locations by crispr RNA (crRNA).
In all, the researchers demonstrated the utility of the CRISPR-Cas9 system as a programmable ‘molecular scissor’ that could cut in DNA at a chosen spot with unparalleled accuracy. The specific spot could be picked by modifying the crRNA accordingly.
The next year, two teams, led by Feng Zhang and George Church, showed that CRISPR-Cas9 could be used to edit the genomes of eukaryotic organisms.
This innovation has since spurred a myriad applications, from targeted genetic therapies to agricultural advancements. The 2020 Nobel Prize didn’t only honour the researchers: it also symbolised the start of a time in which people couldn’t just read human genomes but also edit or modify the genetic code, with potentially long-lasting impacts on the future of medicine and genetic engineering.
CRISPR in medicine
In November this year, the national regulator in the U.K., the Medicines and Healthcare products Regulatory Agency (MHRA), approved the use of a CRISPR-based method called exagamglogene autotemcel – sold under the brand ‘Casgevy’ – to treat sickle-cell disease and transfusion-dependent β-thalassemia. The approval came after the MHRA evaluated safety and efficacy data in an ongoing clinical trial in 29 and 42 patients respectively.
In close succession, the U.S. Food and Drug Administration also approved Casgevy to treat sickle-cell disease, rendering it one of the first CRISPR-based therapeutics to be approved by two major drug regulators.
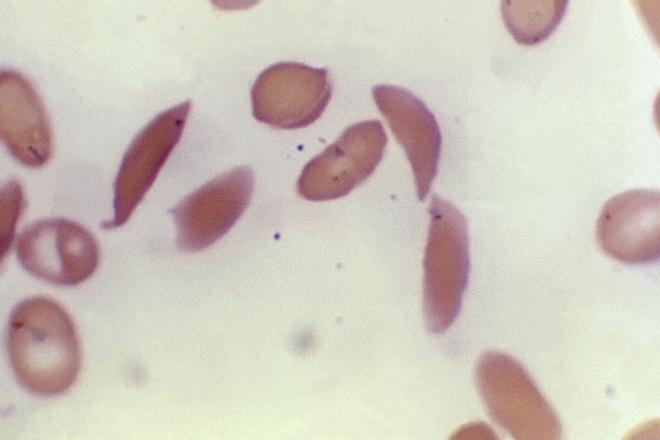
In Casgevy, a patient’s blood stem cells are extracted, their genes modified to remove the defect that produces the sickling, and regrafted back. These cells then proliferate to produce normal red blood cells.
The approvals come full circle 74 years after Linus Carl Pauling described the disease as a molecular disorder. While researchers have developed drugs to treat the symptoms of the disease, Casgevy’s approval signals their ability now to fix its molecular basis.
This said, while these approvals for CRISPR-based therapeutics are exciting, they are all based on what researchers call first-generation technologies. CRISPR-based clinical technologies have grown to become more efficacious as well as efficient, with a panoply of new applications and specificities.
One fascinating approach is called base-editing, where scientists edit genomes at the resolution of a single nucleotide (DNA is a polymer consisting of multiple nucleotides chained together).
Just a few weeks ago, Verve Therapeutics announced results from an important clinical trial it has been conducting to test a base-editing approach to treat familial hypercholesterolemia, another prevalent and oft-undiagnosed genetic disease.
Yet another emerging technique is prime editing, where researchers use a search-and-replace strategy to directly write or insert specific sequences into an existing genome with high accuracy. A fourth example is of systems that use CRISPR to modify epigenetic effects (effects of a body’s environment on its genes) in targeted fashion.
Just the start
None of these technologies are without caveats. Researchers have already reported several safety and accuracy issues. An important one is off-target events: where a CRISPR-Cas9 system becomes inaccurate and edits some other part of the genome, with unintended consequences.
So while there is enormous potential for these technologies, the risk needs to be balanced with both short- and long-term benefits. Many of these therapies are also too early in their development cycle. Continued scrutiny and surveillance may yet reveal ‘side effects’ that we aren’t aware of today.
This said, we can still celebrate what Casgevy et al. mean for the millions of people suffering from genetic diseases, including those whose molecular mechanisms remain unknown. The future has arrived, and it looks remarkably promising.
The authors are senior consultants at the Vishwanath Cancer Care Foundation and adjunct professors at the Indian Institute of Technology, Kanpur.







