Monkeypox was a neglected disease until early this year, with few reports on cases, and that too from travellers, though the disease was endemic in Central and Eastern Africa for many years. First identified in 1958 as a disease in imported monkeys in Denmark, monkeypox is a zoonotic viral infection that can infect humans and other animals. The origin and source of the disease are however unknown, therefore the name ‘monkeypox’ remains a misnomer for the disease.
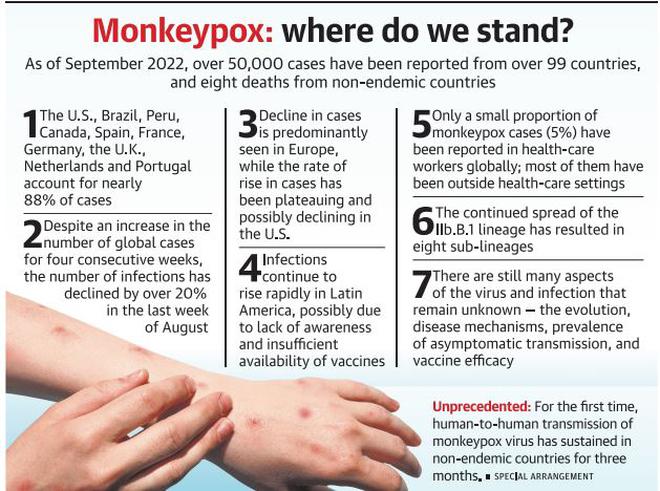
The identification of a cluster of cases associated with a superspreader event in Europe in May-June this year and the subsequent rapid spread across the globe prompted the World Health Organisation (WHO) to declare the outbreak of monkeypox as a Public Health Emergency of International Concern (PHEIC). As of September 2022, over 50,000 cases of monkeypox virus infections have been reported from over 99 countries. Over 15 deaths attributable to the disease have been reported, eight of which were reported from locations that have not historically reported monkeypox, including one from India.
Global situation
As of September 2022, 10 countries account for a majority of cases (over 88%) — the U.S., Brazil, Peru, Canada, Spain, France, Germany, the U.K., Netherlands and Portugal. The disease has predominantly affected males aged between 30-43 years, although demographics have been found to differ between regions. For instance, in West and Central Africa, a larger number of cases are reported among younger individuals.
Declining in Europe
Despite an increase in the number of global cases for four consecutive weeks, the number of reported monkeypox virus infections across the world saw a decline by over 20% in the last week of August 2022. This decline is predominantly attributable to the decreasing number of reported cases in European countries.
Since the beginning of the outbreak, European countries have cumulatively reported over 20,000 cases of monkeypox, including two deaths reported from Spain. The first case of the outbreak in the region was reported in the United Kingdom in May 2022 in a man with a travel history to Nigeria. Heightened awareness and public health measures including vaccination could account for the observed decline.
As cases show a declining trend globally, numbers continue to rise in the U.S. Cumulatively, the U.S. accounts for over 30% of all the global cases, with over 18,000 infections reported from the country to date. The first death in the U.S. linked to monkeypox was reported from the state of Texas. Although the case is still being investigated by health officials to ascertain the role of monkeypox in the death of the patient, early reports from the country state that the individual was severely immune-compromised. A small proportion of pediatric cases of monkeypox have also been reported from the U.S. and with the increase in cases in the country, it is likely that more cases will be found in young children and other vulnerable groups.
Although case numbers continue to increase in the U.S., the rate of rise in cases has been plateauing, and possibly declining. In recent weeks, major cities in the U.S. including New York, San Francisco and Chicago have been showing a decline in cases following the trend in Europe. Like in Europe, this decline may be attributable to the impact of vaccination campaigns coupled with behavioural changes and heightened awareness among people who are at high risk, although more data in the coming days will reconfirm the trend.
Despite a slow decline in cases globally, monkeypox cases continue to rise rapidly in Latin America, possibly also compounded by the lack of awareness of the disease and insufficient availability of vaccines. Amongst all countries in the region, a majority of cases have been reported from Brazil and Peru and a total of three deaths have been reported from Brazil, Ecuador and Peru, although the Peruvian case is still being investigated to confirm monkeypox as the cause of death. Peru is also the third-highest in the world in terms of monkeypox infections per million inhabitants.
Currently, only a small proportion of cases of monkeypox (5%) have been reported in health-care workers globally, although most of the cases were reported to have acquired the infection in the community. Only three cases of monkeypox have been attributed to occupational exposure so far, however additional investigation will be needed to ascertain the risk of healthcare-associated transmission.
Tracking variants
As genomic surveillance continues to provide opportunities to track the evolution of the monkeypox virus, the WHO has laid down the process of naming different variants of the virus taking into consideration the proposals put forward by scientists for a non-discriminatory nomenclature system. Following the new nomenclature, the monkeypox virus variant formerly known as the Congo Basin or Central African clade will be denoted as Clade I, while the former West African variant, which is the main circulating clade in the current outbreak, will be denoted as Clade II. Clade II of the monkeypox virus encompasses two subclades, denoted as Clade IIa and Clade IIb.
The continued genomic surveillance of monkeypox has now resulted in over 1,500 genomes available in the public domain which provides unique insights into the evolution and spread of the virus. At least two distinct lineages of the virus are known to be circulating in the present outbreak. The European outbreak was largely contributed by the IIb.B.1 lineage of virus, but a distinct but smaller lineage (IIb.A.2) presently encompassing genomes from India, the U.K., the U.S. and Thailand was also identified. This lineage has a possible origin predating the European outbreak and possibly had a cryptic spread for almost a year. The continued spread of the IIb.B.1 lineage which encompasses the majority of the genomes has resulted in many sub-lineages — over eight, including the recent one designated from Peru (B.1.6), the U.K. (B.1.7) and Germany(B.1.8).
The present monkeypox outbreak, while may have seen many learnings from the ongoing COVID-19 pandemic put to practice, has exposed many gaps as well. Even as case numbers are brought under control in European and North American countries, global efforts will be needed to contain the spread of the virus in regions such as Latin America and Africa.
Necessary steps
Continued surveillance will be key to preventing future outbreaks of the disease while more in-depth science would be required to understand the pathogen, evolution, disease mechanisms and vaccine efficacy more closely. For example, the quantum of asymptomatic monkeypox transmission and the efficacy of vaccinia vaccine in preventing spread would be of immediate importance. The present outbreak, while calling for global unity and co-operation has unfortunately also put many of these concepts to test. The unavailability of vaccines in Africa which needs it the most, despite the frenzy by rich governments to corner a larger proportion, if not all of the vaccine produced, also puts into question the sincerity in efforts for global health and equity.
As we look forward to fighting more outbreaks in the future, we should keep in mind that nobody is safe until everyone is.
( The authors are researchers at the CSIR Institute of Genomics and Integrative Biology (CSIR-IGIB) in Delhi. All views expressed are personal.)

.png?w=600)



