
Genomic sequencing has been a key tool throughout Aotearoa’s COVID-19 pandemic, with data generated here now part of the 8.5 million genomes shared globally.
It has helped us understand how cases arrived here and the extent of community outbreaks. It has also given us detailed insight into how the virus is transmitted from person to person, on a plane or quarantine facility.
As Omicron spreads rapidly across the country, it is important to consider how we best deploy genomics to achieve our public health goals. Which cases should we sequence and why? What is the role of wastewater when we know cases are already in our cities and regions?
Even as our testing and genomics capacity gets overwhelmed by the sheer number of cases, sequencing will continue to play an important role.
Firstly, we need to keep an eye open for new viral variants and keep track of those already circulating in the community. This is a core role of genomic surveillance and part of a global effort, with scientists around the world sequencing variants in their backyard.
Read more: How COVID-19 transformed genomics and changed the handling of disease outbreaks forever
One thing we are looking for is changes (mutations) in the virus that may affect its ability to transmit, evade our vaccines or immune defences, or cause even more serious disease. Particular scrutiny is given to mutations in the viral spike protein, on the outside of the virus, which allows it to latch onto cells and infect them.
The Pfizer vaccine we have used in Aotearoa essentially presents the body with a copy of the spike protein to train the immune system to create antibodies and other defences against it. Major changes in the spike might allow the virus to evade at least the first line of our immune defences — as we have seen with the Omicron variant, which contains more than 30 different mutations in the spike protein.
The viral arms race
With relatively few cases overall in New Zealand, and only the Delta variant that has persisted in the community for more than a few months, we have so far not seen any concerning new mutations or variants arise here. But small mutations or deletions in the virus’s genetic code remain helpful for linking clusters and detecting new introductions into the community.
The majority of New Zealanders are now vaccinated, which means there is increasing pressure on the virus to escape our immunity. This is an arms race we have been playing with viruses for millennia. The game has changed somewhat as genomics allows us to watch viral evolution in real time.
By sequencing the virus from individual cases, we can tell exactly which variant the person has and, over time, we can detect patterns of variants rising in frequency or resulting in a more severe infection.
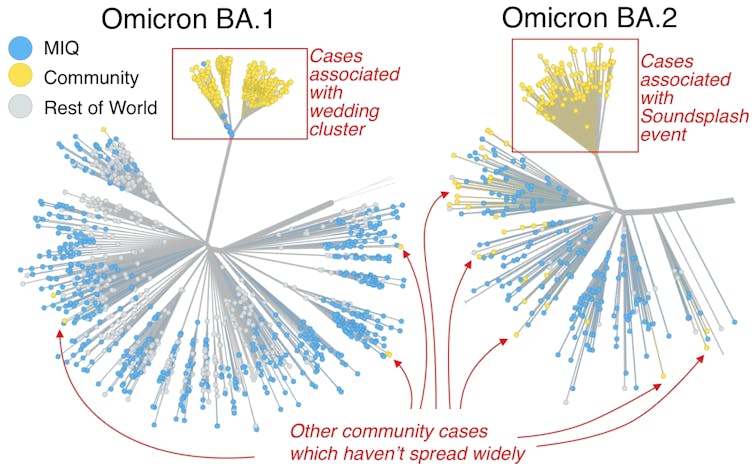
Currently, genomic surveillance tells us there is a mix of Omicron (including major variants BA.1, and BA.2) and a stubborn tail of Delta.
The BA.1 lineage was given an early boost at a wedding-related super-spreading event and now makes up 74% of Omicron cases. The remaining 26% of Omicron cases are BA.2 which was spread early on at the SoundSplash festival. In the last week, about 7% of cases sequenced were Delta. Without sequencing, we would be blind to this.
To maintain high-quality surveillance in the face of very high case numbers, we need to be selective in which samples we sequence and balance competing priorities. The top priority is the prevention of severe disease and there will be a focus on the genomes of cases in hospital. Overseas, many of the serious, hospitalised cases are Delta, not Omicron.
New variants of concern
Some patients may have the misfortune of chronic COVID-19 infections. In such cases, multiple samples may be sequenced to see if the virus is changing within a single patient.
A leading hypothesis of how variants of concern such as Omicron and Delta have emerged is via chronically infected patients who act as an incubator for the virus. We need to continue monitoring patients with long-haul COVID.
We will also need to continue to monitor and sequence new cases that arrive at the border, either in MIQ or in recently returned travellers who test positive. Nearly all the genetic variation of SARS-CoV-2 we have seen in Aotearoa has been imported (as opposed to developed here), and this is a common pattern we see with other diseases such as influenza. By sequencing border cases, we get an early view of what we may need to prepare for.
Read more: Genomic sequencing: Here's how researchers identify omicron and other COVID-19 variants
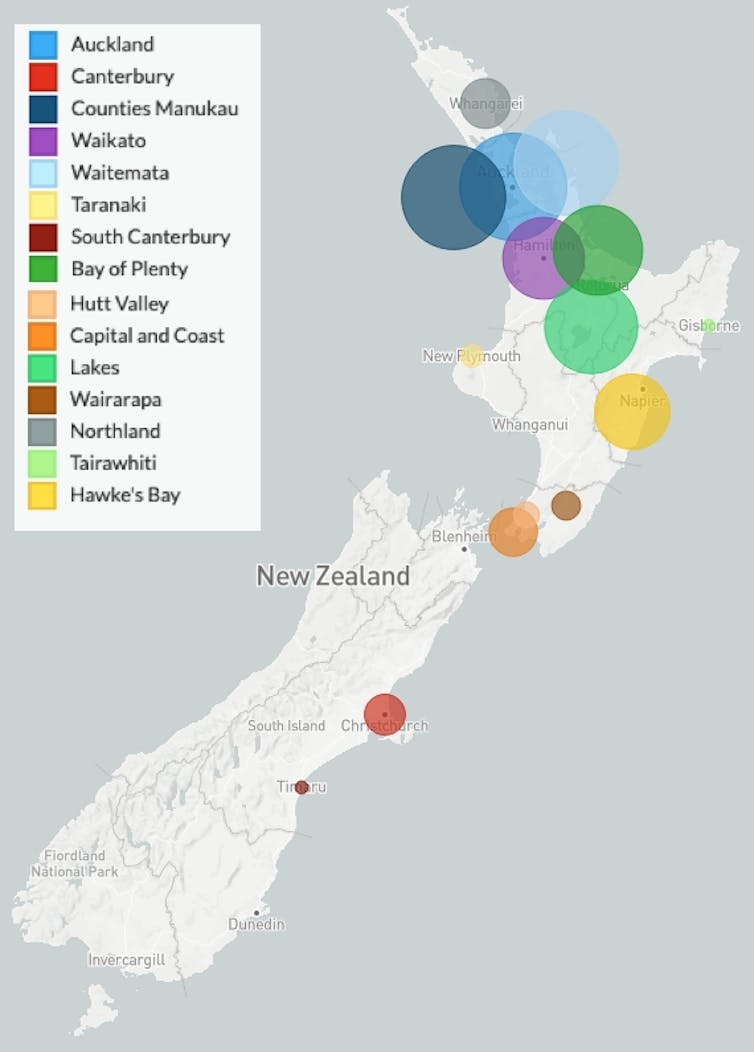
Finally, to get a high-level view of cases and mutations, we sequence a random sample of cases across the country. Genomic sequences taken across time and space build a picture of which parts of the country are host to which variants and lineages. It is very much a case of “know thy enemy”.
Currently we are monitoring the areas where Delta is persisting. We can also monitor how the vaccine status of an individual affects the variant that is detected. Such data helps to build a picture of vaccine efficacy and population-level protection against a fast-changing virus.
Wastewater testing
The last piece of the genomic sequencing puzzle is wastewater testing for SARS-CoV-2. While sequencing from wastewater samples has been used for specific public health investigations in the past, low case numbers and quantities in most wastewater samples has made it difficult. Instead, wastewater testing has focused on using a sensitive method to allow for the early detection of the virus.
With the Omicron surge, we are now seeing an increase in both the number of positive wastewater samples and the amount of virus in those samples. This means we can use wastewater to indicate increasing or decreasing trends in cases at community level, and also to monitor known and new variants through sequencing and other tools.
In the weeks to come, there will be enough viral matter to make trends in wastewater data evident. In some cities, where regular sampling occurs, we will see viral wastewater loads trending up and down with case numbers. This information, along with regular case reporting, will inform the public about the relative risk of various regions. Such data may help people to understand the risks of travelling to a certain region or city.
Genomics remains a key tool in our pandemic management. There will be changes in how we use it, but it remains a core part of our surveillance toolkit. Prior to the genomics era, changes in the viral genetic blueprint were invisible to us. While many will dread another story about a new variant, we would be in a far worse position without this information.
If we step outside of our COVID-19 bubble for a second, the use of fast and affordable genomic technology in this pandemic also provides a glimpse of what genomic medicine may look like in the future — but that is a discussion for another day.
David Welch a previously received funding from MBIE and Ministry of Health.
James Hadfield has received funding from the Ministry of Health.
Jemma Geoghegan works for the University of Otago and ESR. She receives funding from Royal Society Te Apārangi and the Marsden Fund. She has previously received funding from MBIE.
Joep de Ligt works for ESR. The covid genomics is funded through the Ministry of Health and he previously received research funding from the Ministry of Business and Innovation.
Michael Bunce works for ESR. He was previously employed at the Ministry of Health in the COVID-19 directorate.
This article was originally published on The Conversation. Read the original article.







